Diagnosis
Diagnosis of Lyme disease is made through a clinical decision making process that includes a medical history, physical exam, review of past diagnostic tests and consultations, and results from newly ordered tests. In early Lyme disease, one can make the diagnosis of Lyme disease with near 100% certainty when the expanding red rash is present. When faced with a patient with an expanding red rash from a Lyme-endemic region, physicians should draw the conclusion that this is most likely an erythema migrans Lyme rash and start antibiotic treatment immediately; they should not wait to see the results of a blood test, as in early Lyme disease the test is negative 50-65% of the time. Why? Because it can take two to three weeks before the antibodies develop.
With the later disseminated manifestations of Lyme disease, blood tests have a more important role, because by then antibodies will have had time to form. While not everyone with Lyme disease will test positive on currently available tests (e.g. only 70-90% sensitive in neurologic Lyme disease), the tests are very helpful in providing additional information to the clinician to help him/her to determine if Lyme disease is the correct diagnosis.
When starting to evaluate a patient, it is important to obtain a full medical history, including exploring whether or not the person has ever lived or vacationed in a Lyme endemic area. Certain risk factors will increase the risk of tick attachment; these include hiking in the woods or walking through tall grasses or having a pet that might serve as a "tick drag" unwittingly bringing ticks into the house. Certain parts of the United States, such as the eastern states from Maine extending down the Atlantic and upper mid-western states have the heaviest burden of Bb-infected ticks; the Pacific coastal states have also seen a rise in Lyme disease. Because people travel to Lyme endemic areas and because ticks are expanding their geographic range, cases of Lyme disease have been reported throughout the U.S. Lyme disease is a global disease affecting 80 countries, so the initial evaluation needs to ask about travel history; in these other countries, there will be differences in clinical manifestations and disease course because of the varying Borrelia genospecies in these other locations.
The most common testing for Lyme disease is conducted on the blood. However, when central nervous system Lyme disease is suspected, the spinal fluid should be tested as well. When Lyme arthritis is suspected and the fluid in the joint is aspirated, the joint fluid may be tested for evidence of Lyme disease.
Other tests that help with diagnosis include brain imaging tests, neurocognitive tests, tests of the peripheral nerves (nerve conduction studies, small nerve fiber biopsy studies), and tests of autonomic function. When cardiac Lyme disease is suspected, a cardiologist will check heart rhythm on an electrocardiogram and possibly order a Holter monitor. If conduction deficits are noted, the clinician will likely recommend inpatient monitoring in a telemetry unit so that the cardiac rhythm can be closely watched; a temporary pacemaker may be needed if there is a worsening of the heart block.
Blood Tests
Perfect blood tests do not exist. Even with the best tests, some tests will not detect a patient who has Lyme disease (ie, not sensitive enough) or the tests will falsely come back positive in a person who doesn't have Lyme disease (ie, the specificity is poor). Diagnostic test developers aim for tests that combine excellent sensitivity and excellent specificity. That way clinicians won't miss diagnosing someone who does have Lyme disease. Similarly, an optimized test won't lead to inaccurate diagnosis of Lyme disease in people who don't have it.
Understanding the various Lyme tests can be challenging. We devoted 38 pages in the book Conquering Lyme Disease: Science Bridges the Great Divide to clarifying the strengths and weakness of the different diagnostic tests, as well describing the new developments in diagnostic testing. There are indeed new tests under development that will substantially improve the clinician's ability to diagnose Lyme disease.
Clinicians and patients want to know: "Is the infection present in the body?" The clinician is now left with the following options:
Direct Detection Tests
- Culture: The only way of knowing this for sure is if a person is still infected with a living spirochete is if the organism can be cultured. Unfortunately culturing Lyme disease is nearly impossible after the initial infection because the spirochete doesn't stay in the blood or spinal fluid very long.
- PCR: This test looks for evidence of the DNA of Borrelia burgdorferi in the blood or spinal fluid. This test however is not very sensitive for Lyme disease because the genetic material of the spirochete doesn't stay in the blood or spinal fluid very long,
- Antigen detection: This test looks for pieces of the protein of Borrelia burgdorferi. Tests that use this technique have focused on the urine primarily. The assumption is that if pieces of the protein are still present, then the organism has been there recently. This is still considered a relatively experimental test.
Indirect Detection Tests
Antibody-based tests (ELISA, IFA, Western blot, Immunoblot): These tests detect antibodies against Borrelia burgdorferi in the blood or spinal fluid. This is the most commonly ordered set of tests for Lyme disease. The indirect fluorescent antibody (IFA) was the first test developed and is rarely used today as there is considerable subjectivity in the technique. The enzyme-linked immunosorbent assay (ELISA) is more quantitative and automated. The Western blot or Immunoblot can also be read by a clinician or scanned by a machine that quantifies the density of the banding pattern. Several points should be noted:
- It is important to note that these tests do not directly detect the presence of the B. burgdorferi spirochete. Instead, these tests detect antibodies in the blood which have formed in response to the B. burgdorferi spirochete.
- A positive test does not mean that active infection is present. A positive test only indicates that a person has most likely been infected with the agent of Lyme disease in the past or quite recently. The immune response has a long memory; therefore positive tests results may last for many years after the infection is gone.
- A negative test early in infection is meaningless as the antibody response takes time to develop (one to three weeks).
- To a certain extent, these tests suffer from the problem of "cross-reactivity". This means that other microbes (for example a virus or another bacterium) may contain proteins that are similar to the proteins on the Lyme spirochete. The antibodies that are formed to target this other microbe then mistakenly will attach to the protein markers on the Lyme tests — leading to false positive results.
- The biggest problem with these antibody tests is that they do not give information on whether or not infection is present at the time of the test. (However if there is a dramatic increase in an ELISA or a 4-fold rise in titer on an IFA, then it is likely that active infection is present).
- These antibody tests have poor sensitivity in early Lyme disease (35-50%) and inadequate sensitivity in some of the later stages of Lyme disease (e.g, 75-89% in neurologic Lyme disease). This lack of sensitivity could result in a person with Lyme disease testing negative.
- Testing positive on one to three "bands" on the IgG Western blot may not be significant at all. For example, the 41 and 66 and the 93 kDa bands are known as sites on the blots that can attract cross-reactive antibodies initially targeting other microbes. In other words, reactivity on a small number of bands does not necessarily mean one has been infected with the agent of Lyme disease.
In the 1990s, in an effort to improve specificity, the Centers For Disease Control (CDC) adopted the two-tiered strategy for testing. This entails first ordering an ELISA or IFA. If these tests are negative, no further testing is recommended. If either of these tests are equivocal or positive, then the Western blot should be ordered. A positive Western blot could result in either an IgM or IgG result. If the infection is recent and a positive IgM or IgG result is detected, then this is good evidence to confirm recent infection with B. burgdorferi. If the infection is greater than four weeks old, and a positive IgG result is present, this is good evidence of current or previous infection. Because the IgM tests are less specific then the IgG based tests, the CDC recommends not using the IgM for diagnosis if the infection is over four weeks old.
Our experience suggests that physicians should order both the ELISA and the Western blot. In our studies, we found that about ten percent of patients who have a positive IgG Western blot will have a negative ELISA. Given the very high specificity (ie, very few false positives) of the IgG Western blot, it would be unfortunate should a positive IgG Western blot be missed because it wasn't ordered.
Recombinant or Synthetic Antigens: A major breakthrough in antibody-based tests came with the incorporation of synthetic or recombinant antigens into the assays. These are more precise markers of the Borrelia spirochete — representing small areas that are considered less cross-reactive and possibly unique to the Borrelia spirochete; thus, these recombinant or synthetic antigens are less likely to cause false positive cross-reactive results. The first example of this test came in the early 2000s with the C6 Peptide ELISA. While still testing for Lyme antibodies, the sensitivity and specificity of the C6 ELISA were enhanced, representing an improvement over the standard "whole cell sonicate" ELISA. In one study of early Lyme disease, the C6 ELISAwas shown to have a sensitivity of 56 percent compared to 42% for the standard two-tiered test. A similar test is the VlsE ELISA. Both the C6 and the Vlse components add to the enhanced sensitivity of these ELISAs.
Cerebrospinal Fluid Tests
Patients with neurologic symptoms suggestive of central nervous system involvement should have a lumbar puncture with determination of opening pressure. When the cerbrospinal fluid (CSF) is examined, the fluid should be sent for routine studies such as cell count, and protein and glucose levels. In addition, the CSF should be sent for Bb PCR assay and paired serum and CSF should be sent for calculation of the intrathecal index. Please note that the serum should be drawn on the same day as the spinal fluid for an optimal study. The index refers to the ratio of Bb antibodies in the CSF compared to the serum, corrected for immunoglobulin levels in each of those fluid compartments. When the index is positive, that indicates that there is a preferential production of antibodies against Bb in the CSF – a finding strongly suggestive of central nervous system invasion by the agent of Lyme disease. It is believed that the index may remain positive long after the initial infection has been treated due to immunologic memory. If the CSF is being examined as part of the differential diagnosis with multiple sclerosis, the neurologist is also likely to order other tests, such as an assay for oligoclonal bands. Unfortunately, patients may have neurologic Lyme disease but test negative on the Lyme index. When positive however, the clinician can be confident that this particular individual has or has had central nervous system Lyme disease.
Brain Imaging
Magnetic Resonance Imaging
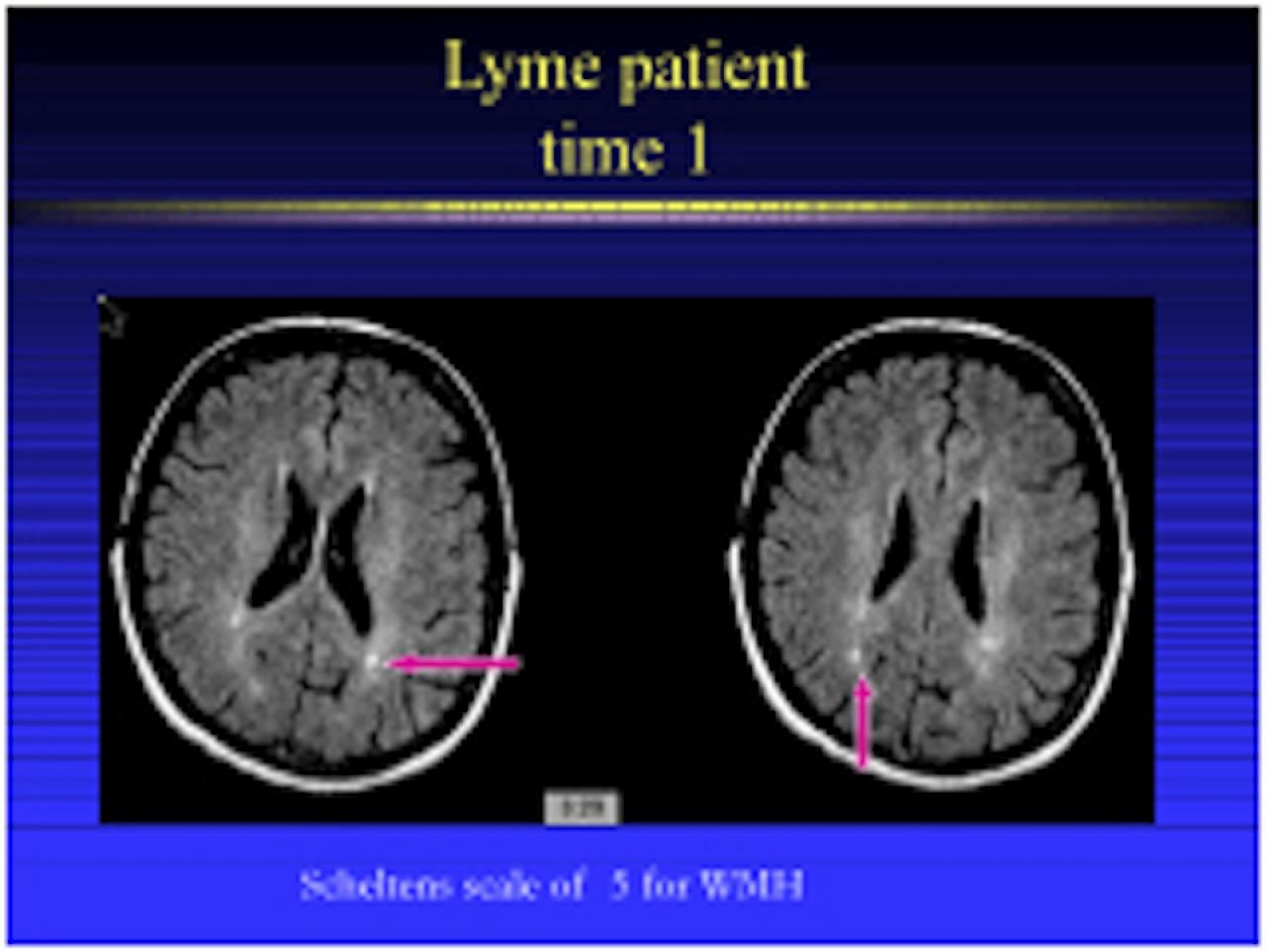
Unlike SPECT and PET images which assess brain function, MRI captures the physical structure of the brain. Inflammatory abnormalities in the brain are also assessed with MRI scans. In children with neurologic Lyme disease, the MRI may reveal white matter hyperintensities suggestive of inflammation or areas of demyelination. Up to 40% of adults with Lyme disease may also have small white matter hyperintensities, but it should be noted that the number of hyperintensities increase with age — even among patients who do not have Lyme disease. In addition, certain factors such as ischemic disease or a history of smoking may result in an increased number of hyperintense areas.
The white matter hyperintensities are sometimes called UBOs or "unidentified bright objects". In some patients, antibiotic treatment results in a diminution or disappearance of these hyperintensities. Certain MRI sequences, such as FLAIR, are best able to detect hyperintensities. These MRI images in Lyme disease may appear similar to the demyelinated areas seen in the "white matter" of the brain MRI of patients with multiple sclerosis. Because an MRI scan uses a very powerful magnet, patients with pacemakers or other metallic implants should not get an MRI.
SPECT Imaging
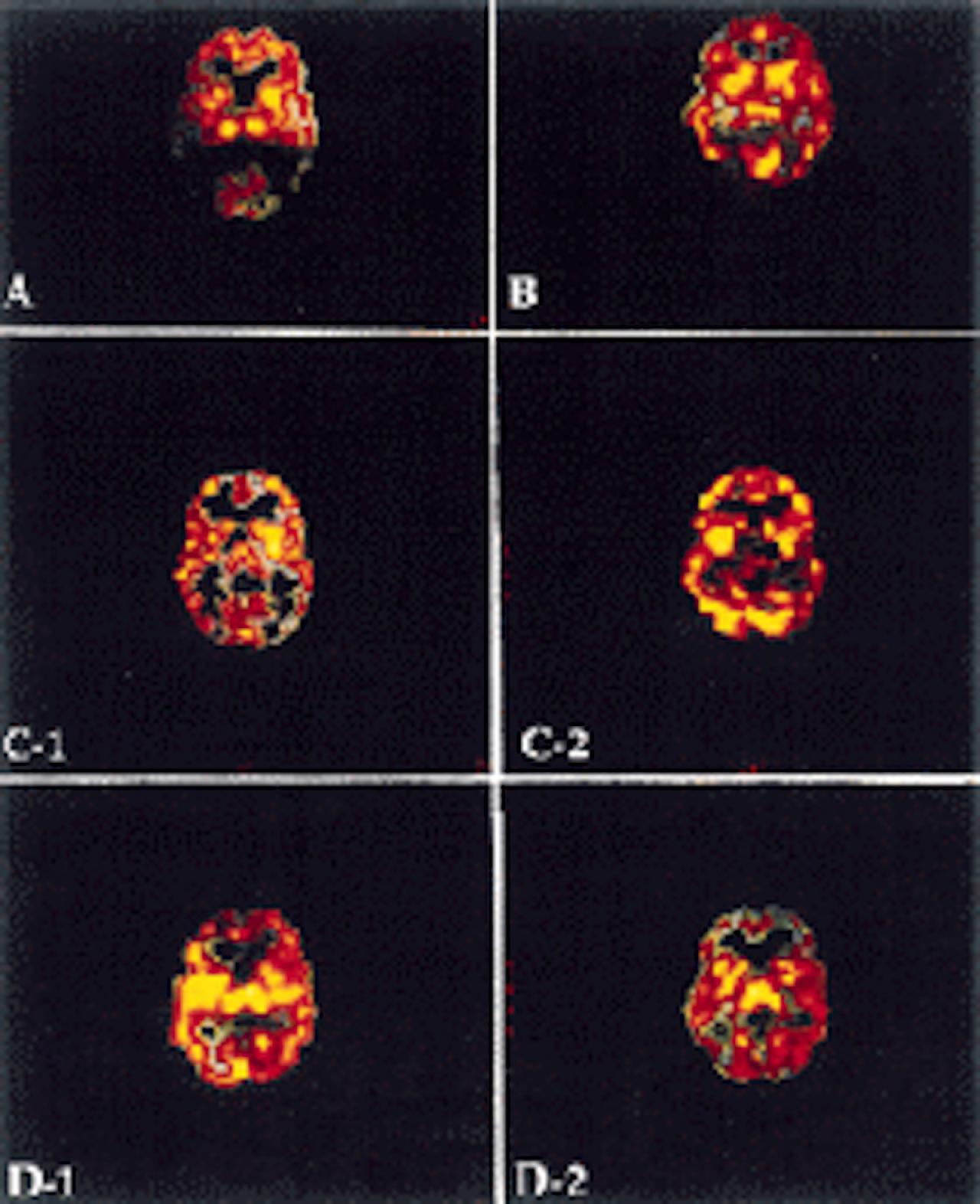
Single Photon Emission Computerized Tomography (SPECT) is an imaging device that provides a picture of the functioning of the brain by assessing blood flow. The advantage of SPECT imaging is that it is widely available and relatively inexpensive (compared to PET imaging). SPECT machines with several "heads" allow for increased imaging sensitivity. In Lyme disease, the most common finding is of heterogeneous hypoperfusion diffusely throughout the brain. This pattern cannot be distinguished from diseases with a similar pattern, such as Lupus, chronic cocaine abuse, or other vasculitic inflammatory disorders. This pattern of heterogeneously decreased perfusion is different from what one would see in patients with primary depression or Alzheimer's disease. Approximately 70% of patients with chronic Lyme disease will have multiple areas of hypoperfusion.
Although the pattern looks like a vasculitis, such a pattern could be produced even if the blood vessels were normal if the nerve connections to the blood vessels were functioning abnormally. In other words, a SPECT scan cannot tell you whether the problem is due to your blood vessels or due to nerve cell dysfunction. SPECT scans also are limited in that the images obtained are rated relative to a part of the brain that is presumed to be working normally, such as the cerebellum or deep gray matter. This may not be true in Lyme disease. This lack of "absolute quantification" limits the firmness with which one can draw conclusions regarding a SPECT image. Although SPECT imaging may be considered a helpful adjunctive tool in the differential diagnosis of Lyme disease, it does not and cannot "make" the diagnosis of Lyme disease.
SPECT imaging is also used to determine whether the heterogeneous hypoperfusion has diminished over time, perhaps due to treatment. Repeated SPECT scans should be done at the same medical center to allow for a fair comparison across images.
PET Imaging

Different radiopharmaceuticals allows us to measure different aspects of brain function. For example, the most widely used "tracer" for measuring regional brain blood flow is 15O-labeled water.18F(fluorine) as fluorodeoxyglucose (FDG) is widely used to measure brain glucose metabolism, since the brain uses glucose to function. Because the radioactive tracer used for FDG PET scans is stable over many hours, PET scans in clinical settings typically assess metabolism directly (through monitoring of glucose function) rather than blood flow. One way of determining whether the brain blood vessels are functioning normally is to conduct a 15O-PET before and after a carbon dioxide inhalation challenge. The patient is then asked to breathe through a tube that contains a slightly higher amount of carbon dioxide than the normal atmosphere. In a person with normal blood vessels, this should result in an expansion of blood flow throughout the brain. If certain areas have damaged blood vessels, then the expansion of flow in that area would be less. This is one way of determining whether the problem in a disease (such as Lyme encephalopathy) is due to inflamed or blocked small blood vessels or due to normal blood vessels with abnormal nerve input. Because this carbon dioxide inhalation challenge however is not routinely available in the clinical setting, an approximation may be obtained by using the medicine acetazolamide. Positron Emission Tomography (PET), although primarily a research tool, has been used increasingly for clinical purposes. PET imaging can demonstrate biochemical or physiological processes involved in brain metabolism. The assumption behind all functional brain imaging (such as PET) is that there is a close relationship between local brain nerve activity, brain glucose metabolism, and brain blood flow. The advantage of PET (in comparison to SPECT) is that the images have enhanced resolution and, in research settings, with the use of an arterial line, absolute quantification of the metabolism and flow in different brain areas is possible. In other words, unlike SPECT which requires assumptions about normal and abnormal brain areas for interpretation, PET can provide a definitive absolute number regarding the amount of flow or metabolism in a particular area of the brain. Because a PET center requires a highly trained multidisciplinary staff of physicists, chemists, computer and mathematical experts, technologists, and physicians as well as a cyclotron in the same building as the patient and the scanner to allow for production of the radiopharmaceuticals, PET scans are more expensive and far less widely available than SPECT scans.
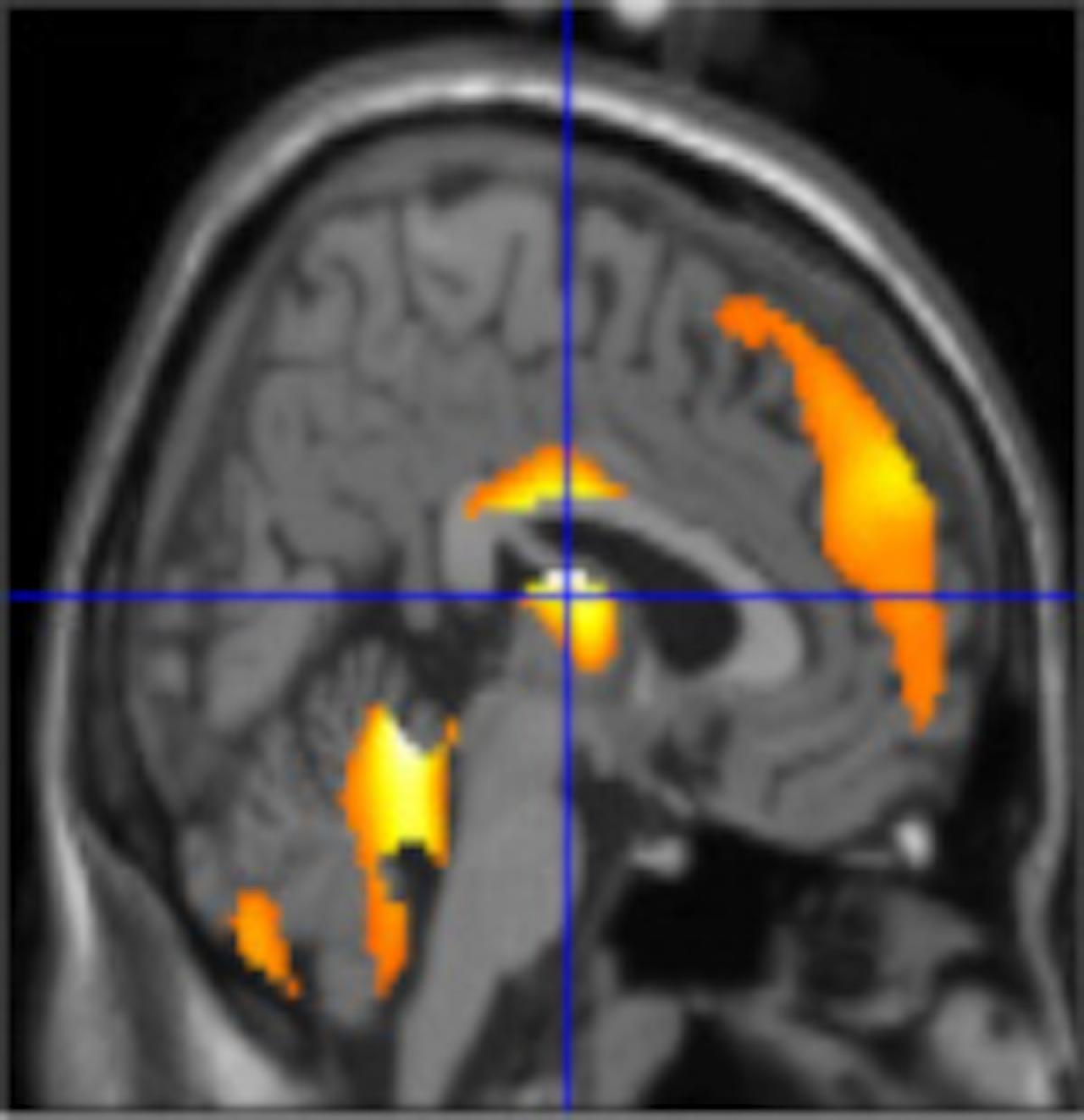
At this point, it is unclear whether PET has an advantage over SPECT for clinical evaluation of a patient with possible Lyme disease. Recent reports from James Moeller, PhD, of the Lyme and Tick-Borne Diseases Research Center suggest that there is a specific neural circuit that can be measured using a PET scan that may be associated with intrathecal antibody production using the C6 ELISA assay. If this finding is confirmed by further study, then PET scans may emerge as a very helpful clinical tool in differential diagnosis.
EMG/Nerve Conduction Studies
Electromyography (EMG) and nerve conduction studies assess the integrity and function of muscle and nerve, respectively. The EMG test allows the neurologist to distinguish neuropathic from myopathic disease and define the precise distribution of muscle involvement. Nerve conduction studies inform the neurologist about the integrity of sensory or motor nerves; an electrical stimulation is applied to the skin overlying a peripheral nerve to enable a recording of the speed of conduction and amplitude of the “downstream” action potential. NCS assist in the diagnosis of nerve disorders, such as demyelinating neuropathy (slow conduction velocity), axonal neuropathy (reduced amplitude of CMAP), and root compressions.
Skin Biopsy
Lyme disease can cause a neuropathy with associated sensory symptoms and sensory loss. To detect small-fiber damage, skin biopsies are now being performed in many diseases that cause neuropathies. In diabetes, some studies suggest that the density of intraepidermal nerve fibers (IENF) is correlated with the extent of the neuropathy and with the duration of disease; lower density correlates with higher neuropathy scores In other systemic diseases, such as Lupus, sarcoid, sjogren’s, celiac, and hypothyroidism, skin biopsy has been used to show a correlation between small-fiber degeneration and neuropathic symptoms. IENF density is a general marker of axonal integrity in peripheral neuropathies, but it cannot be used to make a specific diagnosis. Recently, neurologists have begun to examine patients with Lyme disease to assess small nerve fiber density. The skin biopsy procedure itself is typically performed with a 3-mm disposable circular punch needle with a sterile technique using local anesthesia (2% lidocaine and epinephrine).
Neuropsychological Testing
Comprehensive cognitive assessments are valuable for several reasons:
- They provide an objective measure of the person's cognitive functioning at a specific point in time.
- By providing fully quantitative results, the testing is a very useful way to monitor change in response to treatment for patients with cognitive deficits.
- Tests may help to differentiate between organic or neurologic and psychiatric causes of cognitive problems.
- An understanding of static deficits may help to guide the individual in the construction of alternate strategies to cope with cognitive deficits; for example, a person with auditory attention problems may do best with visually presented information.
Since subjective reports of cognitive difficulties, such as memory problems, do not always correlate with objective data, we cannot rely only on self-reported cognitive problems. A comprehensive selection of tests is administered, including measures of general intellectual functioning as well as specific areas of functioning such as verbal and visual memory and learning, attention/concentration, verbal fluency, processing speed, fine and gross motor functioning, and executive functioning is administered. The sensitivity of neuropsychological tests in identifying brain dysfunction is high, though the test deficits are not specific to Lyme disease. Measures of psychopathology, particularly depression and anxiety are administered as well since affective states may affect cognitive performance .
Impairments in memory, working memory, attention and mental activation, language conceptual ability, and motor function have been documented in adults with Lyme disease. The most consistently identified deficits in adults with Lyme disease have been problems with verbal memory, verbal fluency, and mental processing speed. Verbal memory is typically assessed by a list-learning task such as the Buschke Selective Reminding Test or the California Verbal Learning Test. Verbal fluency is often assessed through the Controlled Oral Word Association Test or through Category fluency tests. Speed of processing is assessed through any of the timed tests, such as digit symbol.
Studies by Keilp, Kaplan, Krupp and others support the hypothesis that cognitive impairments are caused by CNS dysfunction and not secondary to a psychological response to chronic illness. Subjective memory impairments may however be higher in Lyme disease patients with comorbid depression, a finding which strengthens our recommendation that patients with depression should be monitored closely by a psychopharmacologist.